
While all clinics agree that care quality should always be improving, that ambition often runs into the same set of obstacles: fragmented data, inconsistent processes across teams, communication gaps, and operational inefficiencies no one owns.
The result is familiar — improvement initiatives happen in bursts, usually triggered by an inspection or a complaint.
The good news is that the toolkit for sustained quality improvement (QI) is well established. It doesn't require new technology or expensive consultants to get started — most of these tools and methods are low-barrier, operational, and designed for busy clinical teams.
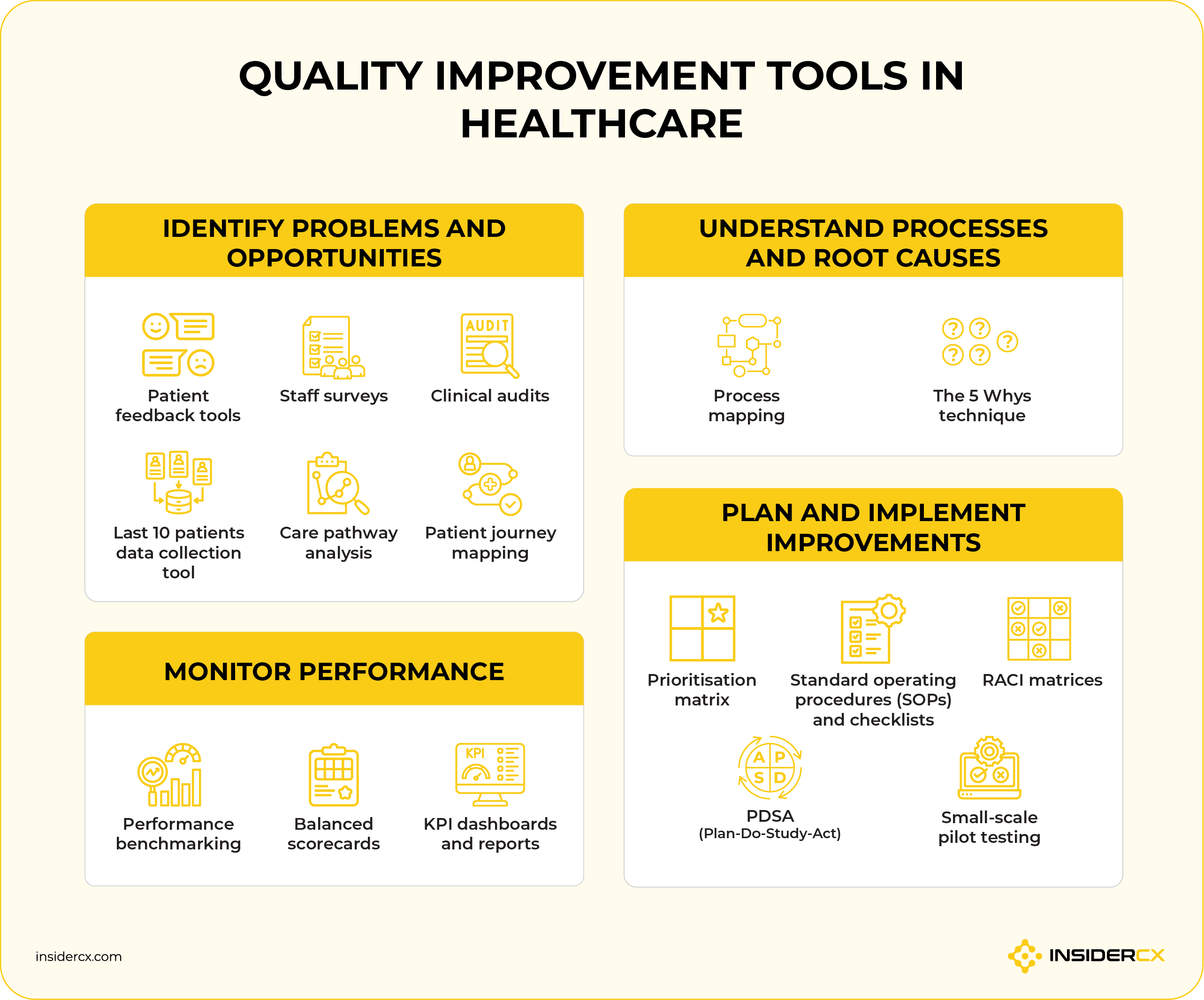
This article walks through the ones that deliver the most value in private healthcare settings, organised around the four jobs a healthcare quality management programme needs to do: identify problems, understand causes, plan improvements, and monitor performance.
1. Tools for identifying problems and improvement opportunities
You can't fix what you can't see. This first category of QI tools exists to surface issues, preferably before patients or regulators do. The organisations doing this well combine input from patients, staff, and clinical records, since each source reveals a different layer of the same operation.
Patient feedback tools
Patient feedback is the most direct line of sight a clinic has into how its service is actually experienced. It tells you which parts of the patient journey your patients are satisfied with, and more importantly, where the quality and operational gaps are that you need to address.
Useful feedback typically comes from the following channels:
- Post-visit feedback surveys: Short, structured surveys sent shortly after the appointment, usually by SMS or WhatsApp.
- Telephone interviews: Deeper qualitative conversations, often used after complex procedures or for high-value patient segments.
- Online reviews and comments: Public ratings and comments left on Google, TrustPilot, Facebook, and healthcare review platforms.
- Submitted complaints: Formal complaints received through the clinic's own complaints system (be it via email, telephone, paper form, or a feedback platform).
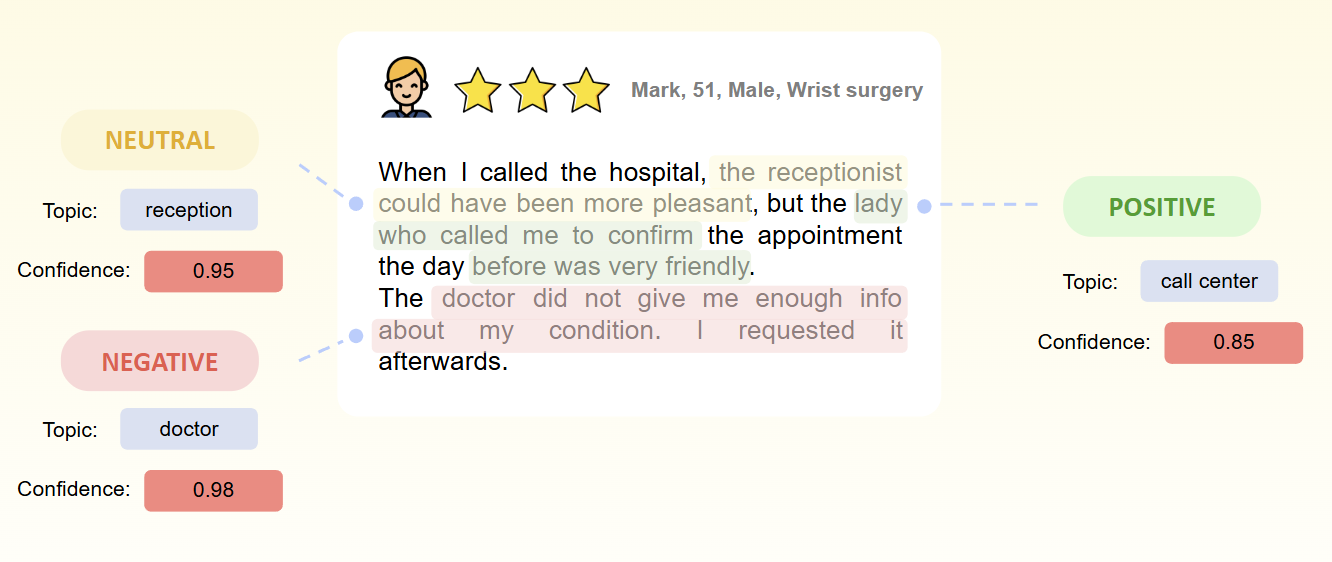
The challenge is volume. A clinic seeing a few hundred patients a week will quickly generate more open-text comments than any team can manually review. Sorting them by hand is slow, inconsistent, and tends to miss the patterns that matter most.
Patient feedback platforms like InsiderCX are designed to automate this at scale. AI-powered sentiment analysis automatically tags each comment by theme and sentiment. Leaders can check the real-time dashboards to see which topics are trending up, which are deteriorating, and what are underlying drivers of those changes.
Staff surveys
Staff usually see problems before patients do. Tapping into that knowledge is one of the highest-leverage things a clinic can do.
A few practical pointers for effective staff surveys:
- Keep them short: Five to ten focused questions get more honest answers than a thirty-question audit.
- Protect anonymity: Without it, you'll get the answers people think you want to hear.
- Run them on a predictable cadence: Quarterly works for most clinics, annual is too slow to catch emerging issues.
- Always close the loop: if you ask and don't act, response rates will collapse over time.
Clinical audits
Clinical audits compare what your team actually does against a defined standard — usually a clinical guideline, internal protocol, or accreditation requirement. They are particularly useful after a process change, when introducing a new pathway, or as part of a regular compliance cycle.
When done right, audits are a quality improvement tool rather than a policing exercise. Done badly, they generate paperwork and resentment. The difference usually comes down to how findings are communicated and whether staff have a clear path to act on them.
For a deeper walkthrough of the audit process — including scope, sampling, and how to report results — see our guide on how to do a clinical audit.
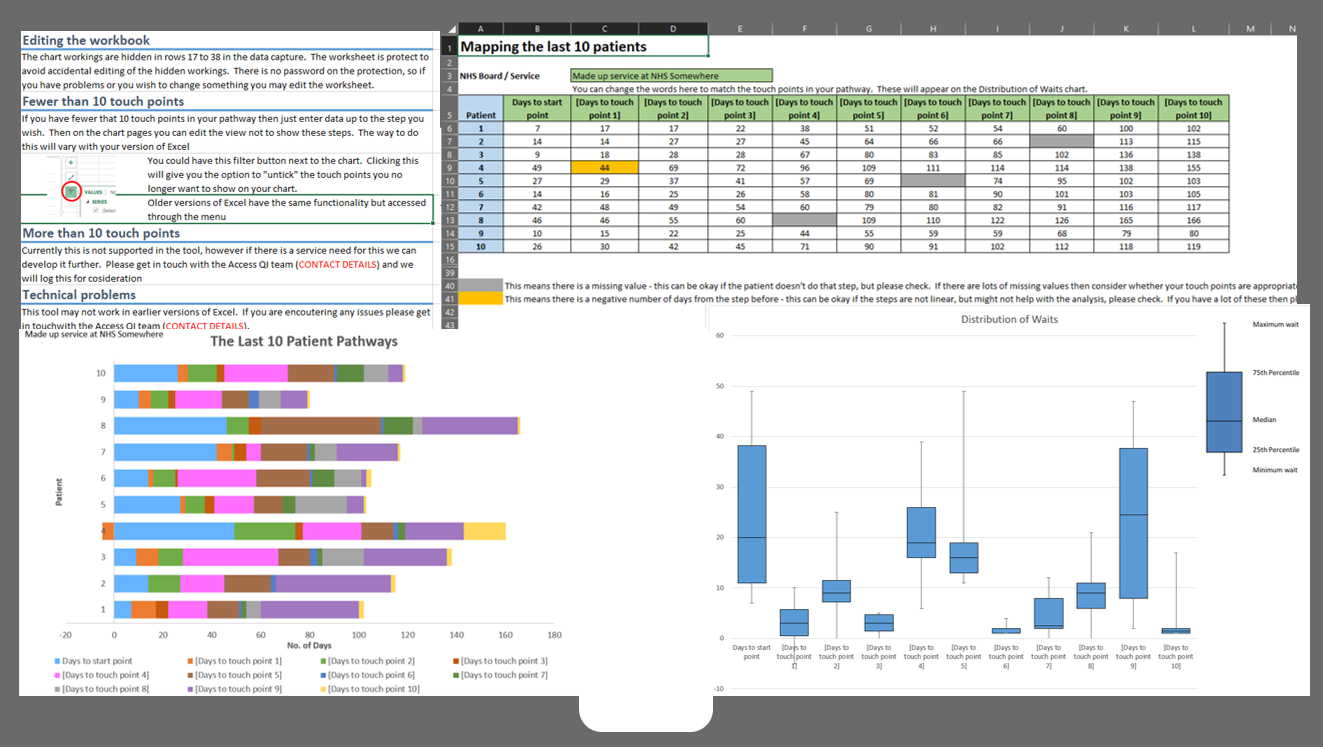
Last 10 patients data collection tool
The original idea behind this technique is to have a structured way to understand patient flow within your care pathways and identify your longest wait times. It complements both conventional process mapping and value stream mapping. Here’s a guide on how to conduct it.
The same idea can be replicated in simpler form for other areas: pick a specific process — say, post-operative follow-up calls — and pull the records of the last ten patients who should have received that call. Check whether each one did, and to what standard (i.e., which questions were asked, what information was provided).
It's fast, low-cost, and grounded in real cases rather than aggregate averages. A team can run a "last ten" check in an afternoon and walk away with concrete examples of where the process held up or where it broke down.
Used this way, it's ideal as a spot-check between formal audits, or as a first look at a problem area before committing to a larger investigation.
Care pathway analysis
A care pathway is the standard sequence of clinical and operational steps a patient moves through for a specific condition or procedure — for example, the full journey of a hip replacement patient from initial referral to final follow-up.
In the context of quality improvement, care pathway analysis can be applied to map out the sequence, then look for variation, delays, or steps that don't add value. It's particularly useful when outcomes are inconsistent across patients receiving the same treatment, when waiting times are creeping up, or when handovers between specialists feel unreliable.
Quick example: A cardiology service suspects that follow-up adherence varies widely between patients. Mapping the pathway reveals that some patients are booked for follow-up at discharge, while others are expected to call the clinic themselves. Standardising that single step lifts follow-up adherence rates without adding clinical capacity.
Patient journey mapping
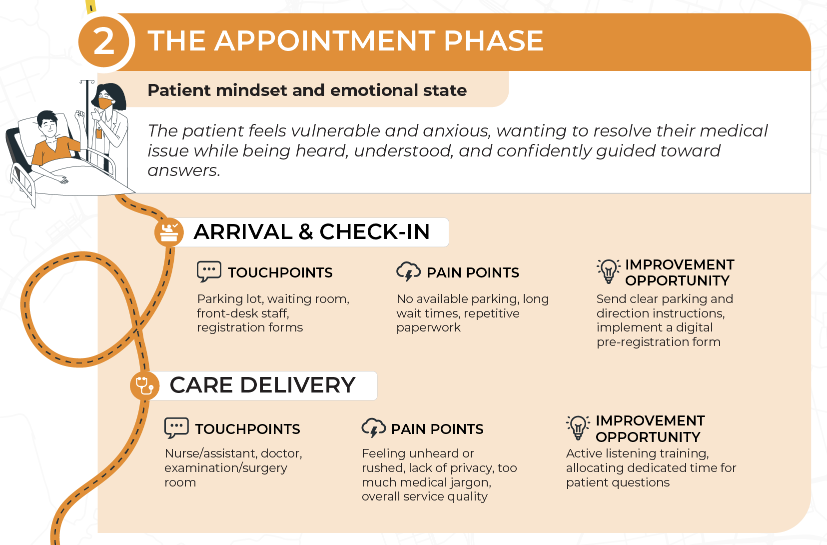
Patient journey mapping looks similar to care pathway analysis but answers a different question. Where the pathway describes the clinical steps, the journey describes the patient's experience of those steps — what they think, feel, and struggle with at each touchpoint.
Here’s a quick snippet from our patient journey mapping infographic to give you a better idea of what it focuses on
Use it when there's a gap between what the clinic believes it delivers and how patients describe their visit, or when satisfaction scores point to a problem nobody can locate operationally.
Here’s a step-by-step guide for creating a patient journey map if you’re interested in learning more.
2. Tools for understanding processes and root causes
Spotting a problem is only the first step, and acting on the wrong cause is one of the most common reasons improvement projects fail — teams treat the symptom, the symptom recurs, and confidence in the QI programme drops.
The tools in this section help teams trace problems back to their actual source before designing a fix.
Process mapping
Process mapping is the act of drawing out a process — every step, every decision point, every handover — so the team can see it as a whole instead of in fragments. It's deceptively powerful: in most clinics, no single person actually knows the full end-to-end flow of even routine processes like outpatient bookings or prescription renewals.
Let’s say a clinic maps its outpatient appointment lifecycle: enquiry → booking → reminder → arrival → consultation → follow-up scheduling → post-visit communication.
The exercise reveals that follow-up scheduling depends on three different people across two systems, none of whom owns the step formally. The map makes the gap obvious in a way that no individual interview could.
A few things to watch out for:
- Resist the urge to map everything: Start with one process, end-to-end, before adding others. Maps that try to cover an entire clinic become unreadable and stay on a shared drive forever.
- Map the process as it is, not as it should be: The improvement comes from comparing the two later. Mixing them up obscures both.
- Involve the people who actually do the work: Management's version of the process is always cleaner than the real one.
The NHS Institute for Innovation and Improvement has a detailed guide on healthcare process mapping that can be used as a reference.
The 5 Whys technique
Once a problem is identified, the 5 Whys technique is one of the simplest root cause analysis methods to dig past the surface. The idea is exactly what it sounds like: ask "why" repeatedly, as many times as needed (which often ends up around five times), until you reach the foundational cause of the issue that can be acted upon.
Quick example: A clinic notices that 30% of post-discharge patients call back with questions within a week. Applying the method could look something like this:
- Why? Because patients don't feel sure about their aftercare instructions.
- Why? Because instructions are explained verbally at the end of the appointment, and not every patient gets a written summary.
- Why? Because we have no standardised process/guidelines that must include a written summary at discharge.
- Why? Because the discharge template was never finalised and approved after the last process change.
- Why? Because no single person owns the discharge documentation process.
The "underlying problem isn't poor communication; it's an unowned process. That's a fixable issue, and one that wouldn't be obvious from the initial complaint.
The 5 Whys works best on contained, single-cause problems. For issues with multiple contributing factors, there are many other root cause analysis techniques you can use, like Fishbone (Ishikawa) diagrams or Pareto analysis.
3. Tools for planning and implementing improvements
Identifying a problem and understanding its root cause still leaves the hardest part: actually changing how the clinic operates. The tools below are designed to make that step structured, accountable, and low-risk.
Prioritisation matrix
Most clinics have more improvement ideas than the capacity to deliver them. A prioritisation matrix forces a conversation about which to tackle first by plotting each idea against two axes — typically impact (how much it improves patient experience, safety, or efficiency) and effort (time, cost, and disruption to implement).
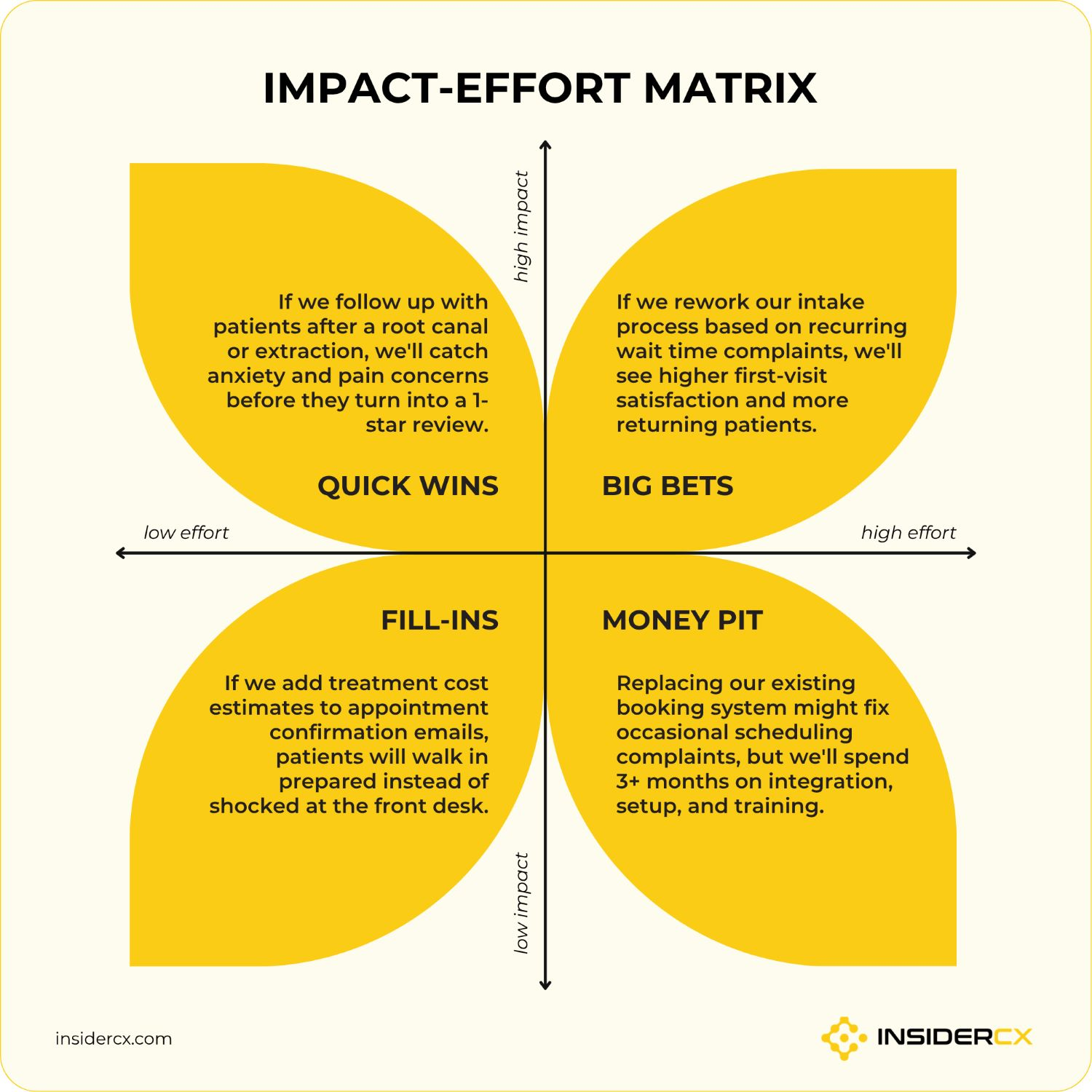
So, imagine a clinic is weighing three ideas: introducing SMS appointment reminders, renovating the waiting room, and switching to digital intake forms.
The matrix makes the decision visible: SMS reminders are low-effort and high-impact, so they go first. Renovation is high-effort and moderate-impact — it goes onto the longer-term roadmap. Digital intake forms sit as medium for both, so they wait until the SMS project is stable.
The impact-effort matrix doesn't make the decision for you. It just makes the trade-offs explicit, which tends to shorten the debate.
Standard operating procedures (SOPs) and checklists
SOPs and checklists are how clinics turn good practice into consistent practice. They reduce variation between staff, accelerate onboarding for new hires, and provide the documentation trail that quality assurance reviewers and regulators expect to see during inspections.
A few principles for using them effectively:
- Reserve them for processes where consistency genuinely matters: Safety-critical steps, high-volume processes, and procedures with handovers between people are good candidates. Creative or judgment-heavy work usually isn't.
- Anchor them in industry guidelines: Whether from a national body, accreditation framework, or specialty association, external standards give your SOPs credibility and make audits easier.
- Match detail to the user: An SOP should give a competent newcomer enough information to perform the task safely and efficiently. More detail than that and it becomes unread; less and it becomes unsafe.
- Review them on a schedule: SOPs that haven't been touched in three years are usually outdated somewhere. Build review cycles in from the start.
RACI matrices
RACI stands for Responsible, Accountable, Consulted, Informed — four labels that, when applied to a process, make role boundaries explicit. It's one of the fastest ways to resolve the recurring "I thought you were handling that" problem in cross-functional work.
Common use cases in healthcare settings include incident response, complaint handling, new service launches, and audit follow-ups — anywhere multiple roles touch the same workflow.
Here’s an example: A clinic builds an RACI for its complaint handling process. The patient experience manager is responsible for managing each case. The clinic director is accountable for outcomes and patterns. The relevant clinician is consulted when the complaint involves clinical care. The front desk team is informed of the resolution so they can answer follow-up questions confidently.
Disagreements about who should be doing what tend to disappear once the matrix is on the wall.
PDSA (Plan-Do-Study-Act)
PDSA is one of the most accessible improvement methods available, in large part because it requires no specialist training. It's designed to handle small, fast cycles rather than large structural changes.
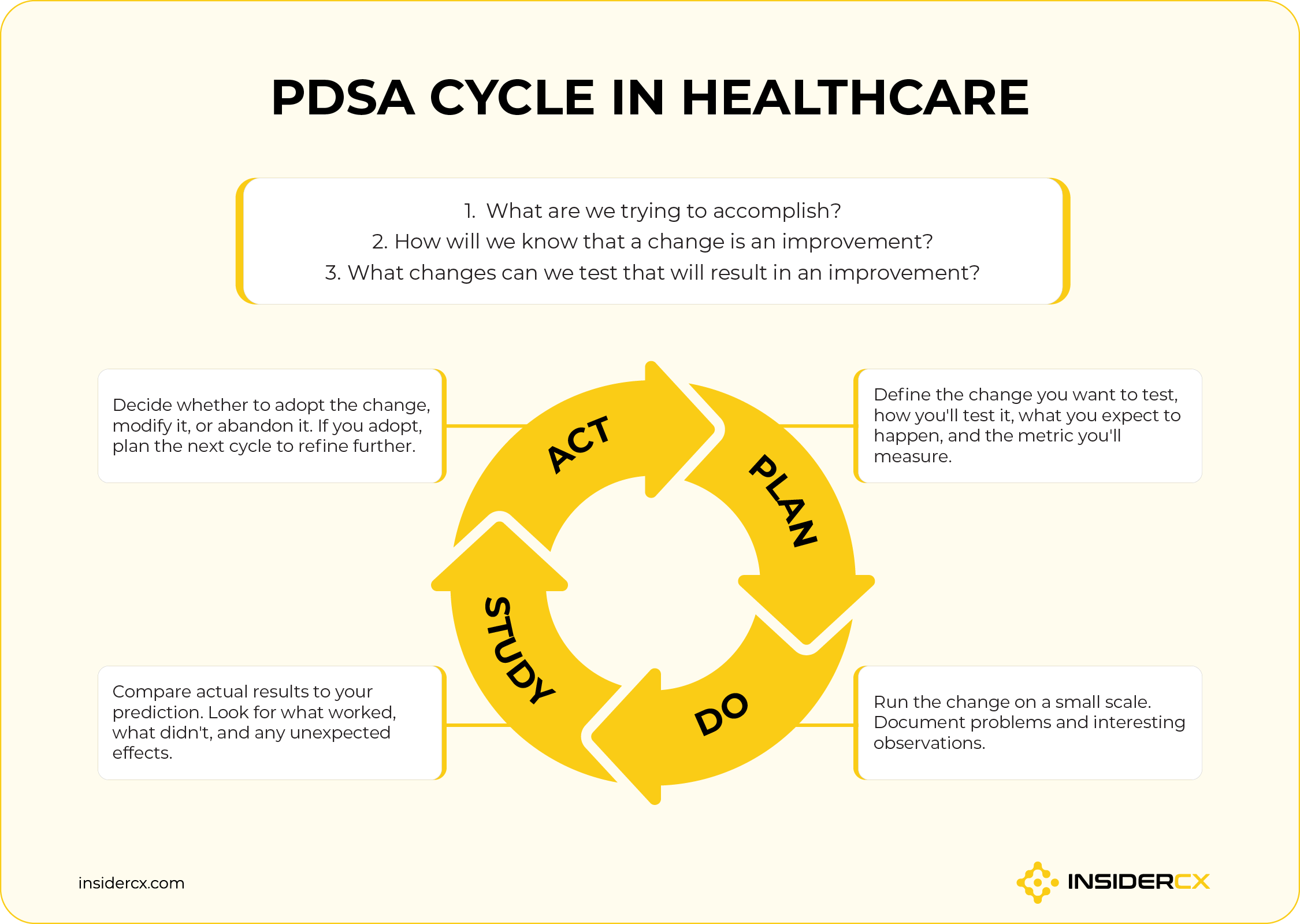
If a clinic wants to reduce no-shows by introducing SMS appointment reminders, here’s what that would look like:
- Plan: Test reminders with two physicians' patient lists over four weeks. Send reminders 24 hours before each appointment. Measure no-show rates against the previous month.
- Do: Send the reminders as planned, log any technical or operational issues.
- Study: No-show rate drops from 14% to 9% for the test group. A small share of patients reply asking to reschedule — a benefit nobody planned for, but worth handling formally.
- Act: Roll out reminders across all physicians, and design the next cycle to test reply-handling workflows.
The strength of PDSA is that it normalises small experiments. Improvements compound across cycles, and the clinic learns to change without large-project anxiety.
Small-scale pilot testing
Pilot testing is, in spirit, the "Do" step of PDSA generalised. The principle is simple: test changes on a small slice of the operation before rolling them out clinic-wide.
The reason is risk management. A new intake form, a revised triage protocol, or a different discharge process can interact with parts of the operation no one anticipated.
Trialling new patient intake forms with a single physician for two weeks reveals practical problems — fields that don't fit clinical reality, instructions patients consistently misread, integration issues with the practice management system — at a scale where they're cheap to fix.
A useful pilot has three features: a clearly defined scope, a fixed end date, and a decision moment where leadership commits to adopt, adjust, or abandon. Pilots that drift on without those produce noise rather than insight.
4. Tools for monitoring performance
Improvement that isn't measured tends to fade. The tools in this section keep change visible — to the team that owns it, to leadership, and to staff who need to see that the work is moving the needle.
Performance benchmarking
Benchmarking gives a numerical context. A patient satisfaction score of 7.8 means very different things depending on what you're comparing it to.
There are two directions worth tracking:
- External benchmarking compares your clinic to industry standards, accreditation thresholds, or published NPS (Net Promoter Score) norms for the sector. It answers the "are we competitive?" question.
- Internal benchmarking compares performance across your own organisation — between locations, between physicians, between services, or between time periods. It answers the "where can we replicate what's working?" question.
For multi-site groups, internal benchmarking is usually the stronger lever. A platform like InsiderCX consolidates patient experience data across locations onto a single dashboard, making it straightforward to see which sites lead in which metrics. Teams stop debating whether differences are real, and start asking what the leading site is doing that the others aren't.
Balanced scorecards
A balanced scorecard is a framework for tracking performance across more than one dimension at a time. The risk it solves is real: optimising aggressively for one metric — say, throughput — often quietly damages another, like patient experience or staff retention.
Healthcare scorecards typically track four categories:
- Patient experience: Satisfaction, NPS, complaint rates, review ratings.
- Financial performance: Revenue per patient, cost per visit, margin trends.
- Operational efficiency: Utilisation, wait times, no-show rates, throughput.
- Staff development: Training completion, retention, satisfaction.

Looking at these together makes trade-offs visible. For quality managers, it can be a tool for evaluating how to continuously improve quality in a more sustainable way.
KPI dashboards and reports
Dashboards and regular reports serve two functions: tracking trends over time so emerging issues get spotted early, and keeping teams aligned on what "good" looks like week to week.
Format varies enormously between platforms. Some clinics use the native reporting of their EHR or patient experience tool; others aggregate into BI tools like Power BI, Tableau, or Looker. Both approaches work; what matters is that the chosen tools can integrate.
A few practical pieces of advice:
- Check integrations before buying: A patient experience or appointment booking platform that doesn’t natively integrate with your CRM or EHR system will create more manual work, not less.
- Limit each dashboard to one audience: Leadership dashboards, operational dashboards, and team dashboards have different jobs; trying to serve all three on one screen serves none.
- Pair every metric with an owner: A trend on a dashboard without anyone responsible for acting on it is little more than decoration.
Digital solutions that can streamline the healthcare quality improvement process
There are many purpose-built tools that clinics can use to streamline different aspects of quality improvement. Plus, most modern healthcare software provides useful data that can be used to support quality decisions and track the effects of implemented changes.
This is why most established QI programmes use a combination of the following software categories:
- Patient feedback platforms: Collect surveys and patient satisfaction data; help identify recurring service issues and track the impact of quality improvement efforts.
- Incident reporting systems: Track safety incidents and near misses; support root cause analysis efforts.
- Audit & compliance management software: Simplify clinical audit scheduling and help clinics organise standards and evidence; useful for general compliance tracking, as well as during inspections and accreditation reviews.
- Workflow and process mapping tools: Help visualise clinic operations and bottlenecks; useful during process redesign projects.
- Business intelligence platforms: Aggregate operational, feedback, and quality metrics; support leadership decision-making.
- Project management and SOP platforms: Centralise policies, procedures, and checklists; improve version control and staff access.
No single clinic needs every category from day one. The right starting point depends on where the biggest visibility gap sits today. For most private clinics, that gap is patient feedback — closing it first usually surfaces the operational issues that justify the rest of the stack.
How the InsiderCX platform support quality improvement in private clinics
InsiderCX is a patient experience platform built specifically for private clinics and clinic groups. It automates the collection, analysis, and reporting of patient feedback across the full patient journey, so quality and operational teams spend their time acting on insights rather than assembling them.
In practice, that means clinics use InsiderCX to:
- Automate feedback collection through SMS and WhatsApp surveys triggered after each appointment, achieving response rates that manual methods can't match.
- Analyse open-text comments at scale with AI-powered sentiment and theme detection, replacing weeks of manual review with structured insight.
- Benchmark performance internally across locations, physicians, departments, and services on a single dashboard.
- Track the impact of improvement initiatives by monitoring satisfaction metrics before, during, and after each change.
- Surface emerging issues early with alerts on negative feedback and shifts in sentiment, before they turn into complaints or negative reviews.
- Generate audit-ready reporting so compliance evidence is available without scrambling at inspection time.
For clinics already working through the tools in this article, the platform tends to fit naturally into the identify and monitor stages — the two places where the volume of data is highest, and where manual approaches break down first.
We have a free pilot project for those who are interested in testing InsiderCX at one of their locations.
FAQs
Which tools are commonly used for quality improvement in hospitals?
The most commonly used tools include clinical audits, incident reporting systems, root cause analysis techniques (such as the 5 Whys, fishbone diagrams, and full RCA reviews), PDSA cycles, process mapping, balanced scorecards, and patient feedback platforms. Larger hospital systems typically layer accreditation and compliance management software on top, particularly where they operate under frameworks like CQC, JCI, or national equivalents.
Can the 7 QC tools be used in healthcare?
Yes — and many of them already are, often under different names. The classic seven Quality Control tools (originally formalised in manufacturing) include check sheets, Pareto charts, cause-and-effect diagrams, histograms, scatter diagrams, control charts, and stratification.
In healthcare practice, Pareto analysis is widely used to prioritise complaint categories or incident types, cause-and-effect (fishbone) diagrams are a staple of root cause analysis, control charts appear in infection rate monitoring and operational performance tracking, and check sheets are the conceptual ancestor of most modern clinical checklists. The translation isn't always one-to-one, but the underlying methods are well-suited to healthcare data — particularly in operational and patient-experience contexts where measurable, repeated processes are the norm.


